 IVF (In vitro fertilisation) was controversial when it was first introduced in the 1970s. Mass protests were held with the slogan “It is against nature and against God!”. Patients were sworn to secrecy for fears of their own safety. Several lawsuits were issued trying to shut the research down. Even the phrase “test tube baby” was meant as an offensive term. Fast forward 40 years, and now IVF is almost as mainstream as a trip to the dentist. Today IVF is responsible for the births of more than five million babies. That’s more people than the entire population of New Zealand. And because global fertility rates are dropping, IVF is only going to become more and more popular.
IVF (In vitro fertilisation) was controversial when it was first introduced in the 1970s. Mass protests were held with the slogan “It is against nature and against God!”. Patients were sworn to secrecy for fears of their own safety. Several lawsuits were issued trying to shut the research down. Even the phrase “test tube baby” was meant as an offensive term. Fast forward 40 years, and now IVF is almost as mainstream as a trip to the dentist. Today IVF is responsible for the births of more than five million babies. That’s more people than the entire population of New Zealand. And because global fertility rates are dropping, IVF is only going to become more and more popular.
Most people know IVF involves taking an egg from a woman’s ovary and fertilising it with a man’s sperm in a lab before putting it back in the woman. However, when it comes to the precise details, very few people actually know what is involved. This can be a problem. Many of my patients have voiced apprehension and anxiety at the thought of going for IVF because they don’t understand what is going to happen and what is expected from them. They are also often unaware that IVF can be performed in several different ways, some which may benefit their particular situation and others that may not. This is why I have devoted this guide to helping you understand what will happen should you choose to undergo IVF.
I’ll begin with the core IVF process, starting with the drugs you’ll take, through egg collection, to the insertion of an embryo. Then I’ll take you through what variations might be included depending on your personal diagnosis or a particular clinic’s practices. Finally, I’ll cover the risks and side effects of IVF and some tips for success.
If you are just starting out, you may also want to read the pages on the beginner’s guide to fertility treatment and how to choose a fertility clinic which you can access by clicking here.
The Core IVF Process
The ‘Welcome’ Pack
When starting a course of IVF, you will be either given or sent a box of goodies (providing your definition of ‘goodies’ is broad enough to encompass needles, syringes and prescription medications). This box contains everything you need to prepare your body for egg collection. Make sure you carefully read any instructions included, as failing to follow the correct procedure could make you seriously ill.
Suppression of Menstrual Cycle
The first step of the IVF process is to suppress your natural menstrual cycle. This resets the cycle and makes the next stage of ovarian stimulation much more effective. This involves taking suppressing drugs for about two weeks. The drugs are self-administered by either injecting them or taking them as a nasal spray.
Ovarian Stimulation
Normally in a natural cycle, ovaries only mature one or two eggs every month. However, when it comes to IVF, most clinics like to encourage your ovaries to mature as many eggs as possible. This gives the clinic a greater number of eggs to choose good ones from. Any extra eggs collected and not immediately used can be frozen in case they are needed later. To encourage your ovaries to produce more eggs than normal, you will need to take a drug called Follicle Stimulating Hormone (commonly known by the abbreviation FSH). This is usually a self-administered daily injection over a course of 10 to 12 days. Do not take more than the recommended dose of FSH. Exceeding the guidelines can lead to Ovarian Hyperstimulation Syndrome (OHSS), which can prove fatal. I will discuss this and other risks in greater depth later on.
If you are interested in seeing an actual injection of FSH, you can watch the video I made of it on YouTube here: Subcutaneous Injection Procedure

Transvaginal Ultrasound Scan
In order to make sure the Follicle Stimulating Hormone is having the desired effect, you may need to have one or more Transvaginal Ultrasound Scans. This is an ultrasound scan performed from within the vagina which is very similar to the pelvic ultrasound scan test for fertility. To learn exactly what this procedure entails, you can read more about it here: Pelvic Ultrasound Scan
Final Hormone Injection
About 34 to 38 hours before they remove the eggs, you’ll have a final hormone injection (usually self-administered) of Human Chorionic Gonadotropin (hCG). This hormone helps the eggs fully mature ready for the next step of retrieving the eggs.
Egg Retrieval Procedure
On the day of egg retrieval, you will need to attend the clinic or hospital where your matured eggs will be removed. This is a minor procedure performed by either a Gynaecologist or a Reproductive Endocrinologist. The procedure is done by inserting an egg collection needle through your vagina and into each ovary. The needle is guided by ultrasound to each mature follicle where the egg and the follicular fluid is sucked out and put into a test tube. The whole egg retrieval process is very quick and only lasts about 15 to 20 minutes. After egg retrieval it is not uncommon to experience some pain in the form of cramps and a small amount of vaginal bleeding.
Normally you will be given a General Anaesthetic for the procedure (commonly referred to simply as a “GA”). This will knock you unconscious so you will not be aware of the procedure. However, it is not unheard of for clinics to offer you a sedation (which takes away the pain, but you remain conscious throughout the procedure).
Preparing the Uterine Lining
After egg retrieval, you are likely to be asked to take the hormone progesterone to help prepare the lining of your uterus. This will help thicken the lining, making it easier for the embryo to attach to and implant. This is commonly a daily pessary which is placed inside the vagina, however, it can be in the form of a self-injection or gel. If you are not immediately asked to take progesterone after egg retrieval, you will likely be asked to take it once the embryo has been transferred back into you. It is normal to keep taking progesterone into the 6th week of pregnancy or beyond. This is because it improves the chances of you maintaining any resulting pregnancy.
IVF Sperm Donation
Around the same time you are undergoing egg retrieval, your partner is providing his contribution in the form of a sperm donation. This procedure is very similar to producing a sample for a semen analysis test, as described here: Semen Sample Analysis. Once the lab receives the semen sample, it is cleaned and the best swimmers are selected for fertilisation with the egg. If your partner is not supplying the sperm, or has done so in advance, then the sperm used is usually from a frozen donation, which is defrosted and prepared in the same way.
Fertilising the Eggs
Once the sperm has been cleaned and the eggs harvested, the sperm is mixed with the eggs in a lab. After approximately 18 hours have passed, the eggs are checked to see if any have been fertilised and become embryos. You may have been told how many eggs were collected during the initial retrieval, but don’t worry if not all of them become embryos. It is perfectly normal for some of the eggs retrieved not to become fertilised.

Embryo Incubation
You may have been led to believe that IVF babies are grown in test tubes. It is simply not true. It is a myth created by the negative media surrounding IVF when it was first introduced. The reality is the eggs that become fertilised are grown in a shallow cylindrical glass or plastic lidded dish called a petri dish. This dish is filled with nutrient chemicals that help the embryo develop.
The embryo is allowed to develop in the container for two to five days before being transferred back to the woman. The precise number of days before the embryo is transferred back depends on the embryo grading. Any spare embryos may be frozen for later use.
Embryo Grading
Not all embryos have the same chance of developing into babies. Embryo grading is a procedure usually carried out by an Embryologist to decide which embryo has the best chance of success of developing into a baby and therefore, which embryo should be transferred back to the woman.
It is important to know that the grade of an embryo is in no way connected to how healthy a baby will be. So, if none of the embryos are graded highly, it does not mean that a baby resulting from one will be unhealthy. It is the DNA which dictates the health of the baby, not the quality of the egg that contains it.
There are two stages in an embryo’s development when it could be transferred to the woman:
- Cleavage Stage – day two or three of their development, sometimes referred to as a ‘day 3 embryo transfer’
- Blastocyst Stage – day four or five of their development, sometimes referred to as a ‘day 5 embryo transfer’

However, not all embryos left to reach blastocyst stage in a container will survive. Whereas, if they had been transferred back into you at the earlier cleavage stage, they might have developed into a pregnancy.
This can leave the embryologist with the dilemma of transferring the embryo earlier at the cleavage stage and potentially not selecting the best one, or waiting until the embryos reach the blastocyst stage and risk losing them. Sometimes, no matter how experienced the embryologist is, it is just luck of the draw.
Embryo Transfer Day
Transferring the embryo back to the woman is a simpler procedure than the egg retrieval process. First, a speculum is inserted into the vagina and a thin catheter tube is passed through this into the uterus. The embryo is transferred into the uterus by injecting it through the catheter. The procedure only takes 10 to 15 minutes and most of that time will be spent first answering questions to make sure they are transferring the correct embryo into the correct woman.
The embryo transfer procedure doesn’t usually require you to be sedated. However, if you have any concerns about being or not being sedated, you should talk to your medical team about them before the embryo transfer day.
After Embryo Transfer
After the embryo has been transferred, you can stand up and walk around. The embryo won’t fall out of you. You can even go to the toilet without having to worry that you will pee the embryo out. Because the procedure can be emotionally tiring, many women like to take bed rest after embryo transfer and this is perfectly okay too.
Common Variations to the Core IVF Procedure
The procedure I’ve described above is the basic IVF procedure. But depending on your situation and the services available at your chosen fertility clinic, there may be certain variations and additions to how that procedure is performed. Bear in mind that most of these extra procedures are likely to cost you additional money if you are undergoing IVF privately. The following are the most common variations and additions:

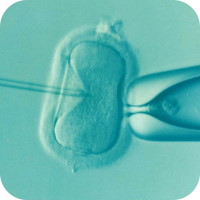
Intracytoplasmic Sperm Injection (ICSI)
Couples don’t just have IVF because the woman has difficulties getting pregnant. IVF is just as good at helping couples where the man is the one with the problem. When this is the case, often an extra procedure is included just before the eggs are fertilised. This procedure is called Intracytoplasmic Sperm Injection, or ICSI (pronounced ‘ick-see’) for short. It is by far the most common procedure to be added to the core IVF process and can help men with all types of fertility problems get their partner pregnant. In this procedure the sperm are viewed under a microscope and the best sperm are selected. Their tail is removed and then the head of the sperm is injected into the egg. This ensures that the sperm’s genetic material makes it to where it is needed.
Low Drugs or No Drugs IVF
When IVF was first introduced, they didn’t use the drug FSH to stimulate multiple follicles for maturing more eggs at the same time. They quickly learned however that by using FSH to increase the number of mature eggs, they could improve the chances of getting a viable egg. The downside to using FSH, and other drugs, is that it has side-effects and risks. Because of this, some clinics offer reduced amounts of drugs compared to other clinics. This has benefits of reducing some of the side-effects and risks, but at the cost of a slight reduction in success rates from these clinics. This is also one of the few variations to the core IVF procedure that is likely to cost you less money than the standard procedure. Deciding whether to go with reduced drugs is often a personal choice, but can be useful for women who are at increased risk of Ovarian Hyperstimulation Syndrome. More on this risk later.
Donor Eggs and Donor Sperm
Having donor eggs or donor sperm is pretty much what you’d expect to see on the side of the tin. For couples where one of the partners cannot provide the genetic material needed to complete a fertilised embryo, a donor substitute may be used instead. These can be either fresh samples, or frozen donations which are thawed out.
Frozen Eggs and Sperm
Sometimes people have their eggs or sperm frozen at an earlier point in their lives. This often happens when there is a risk to their supply of eggs or where the ability to make sperm may be damaged. Examples of this are cancer treatment or genital surgery. Or it can happen when the woman is worried that her egg reserves may be depleted before she is ready to have children. In these cases, the frozen eggs or sperm are thawed out and used the same way as fresh samples.
In Vitro Maturation (IVM)
Normally in IVF, only mature eggs ready for fertilisation are mixed with sperm to turn into embryos. Sometimes the eggs collected are not mature and not ready for fertilisation. In these cases, In Vitro Maturation, or IVM for short, is used to mature the eggs in a laboratory instead of the ovary. The laboratory matured eggs can then be either used immediately or frozen for a later date.
Assisted Hatching
Embryos are surrounded by cells that protect it in a shell. With assisted hatching, a small ‘crack’ is made in this protective shell just before it is transferred back to the women. This is done in the hope that it will help the embryo to better grow in size and increase the chance that it will result in a pregnancy. However, there is a slight risk that this procedure can damage the embryo, resulting in a failed pregnancy. There is also a small increased risk that the pregnancy will result in identical twins.
On the section of the website ‘How to Avoid Fertility Scams and Rip-offs’, I include Assisted Hatching in the list of procedures that lack conclusive evidence that they can improve your chances of getting pregnant. This is because at the time of writing this, there isn’t conclusive proof it improves success rates. This is made more complicated because there are several different ways the ‘crack’ is made in the protective shell layer of cells. These range from chemical methods, to laser, electrical and mechanical. Each method claims to be more successful than the last. Until there is definitive proof that one or more of these methods actually improves the chances of success, I advise that if you are offered Assisted Hatching by the clinic, make sure the clinic tells you of the risks and benefits to your personal situation before you decide to accept the procedure or not.
Other Variations and Procedures
As well as the common variations and procedures I’ve listed above, there are others which are less common or lack scientific evidence. If you are offered one of these, make sure you have read the website page ‘How to Avoid Fertility Scams and Rip-offs’ to better understand whether they are necessary or just another way for the clinic to make money at your expense.

The Risks and Side Effects of IVF
I don’t want to scare you, but every year a very small number of women have complications as a result of IVF treatment. It is not a very big number, especially when compared to the hundreds of thousands of couples that have IVF every year. But the risk is there. The main culprits of IVF related complications are Ovarian Hyperstimulation Syndrome (OHSS) or problems arising from multiple pregnancies. Don’t let it put you off having IVF if nothing else has worked, but it is another reason not to have IVF just because it’s convenient.
In the spirit of full disclosure, let’s take a look at the most common of the risks and side-effects associated with IVF treatment. Do bear in mind that because of the variations in treatment and your personal circumstances, these risks may be greater or lesser for you. Rather than the clinic just handing you a leaflet with them in, have the doctors at your fertility clinic talk through each one with you. And make sure they know you want them explained with your specific circumstances and not just give you a general overview.
Ovarian Hyperstimulation Syndrome (OHSS)
During most IVF treatments, drugs are used to stimulate the ovaries into producing more mature eggs than they naturally would. This can cause your ovaries to become swollen and painful in a condition known as Ovarian Hyperstimulation Syndrome, commonly referred to as OHSS. Mild symptoms of OHSS can range from mild abdominal bloating, abdominal pain, nausea, and slight weight gain. More severe symptoms include rapid weight gain, vomiting, diarrhoea, reduced urine, dark urine, excessive thirst, blood clots, and breathing problems. In extremely rare cases, OHSS can lead to death. Because of the seriousness of these risks, your doctor should discuss these symptoms with you thoroughly before the treatment takes place. And during treatment, should you experience any of the symptoms, even the mild ones, inform your doctor immediately.
If you are at a high risk of OHSS, you may want to consider using a clinic that offers low drugs or no drugs IVF as an alternative.
Reaction to Anaesthesia
IVF involves surgical procedures and like any other surgical procedure that uses anaesthesia, there are risks. Common side-effects include temporary memory loss, confusion, dizziness, nausea, vomiting, feeling cold, and bruising from where a breathing tube was used. In more serious cases, it is possible to have a serious allergic reaction to the anaesthetic. Before going under, your anaesthetist should talk you through these risks and ask if you have had any previous problems with anaesthetic.
Egg Collection Complications
In order to remove eggs, an egg collection needle is inserted into each mature ovarian follicle. This needle then sucks out each egg and its follicular fluid. Despite the needle being guided by ultrasound, very occasionally it can nick or puncture the bowel, bladder or a blood vessel. This can cause bleeding or infection to occur. Usually, the doctor will notice at the time if this happens and you may need surgery to correct it.
Ectopic Pregnancy
Ectopic pregnancy is where an embryo implants itself outside of the uterus. Usually this is in a fallopian tube, but can be the abdominal cavity. When an embryo starts growing outside the uterus, it can cause serious problems. Sometimes it can even result in the death of the mother. Because of this and the fact that it is almost unheard of for an ectopic pregnancy to result in a live birth, these pregnancies are usually terminated to prevent harm. Ectopic pregnancies occur naturally, but IVF treatment has a very slight increased risk of them occurring.
Miscarriage
There is a slight increase of miscarriage with pregnancies conceived using IVF when compared to those conceived naturally. There is a myriad of reasons why a miscarriage could occur, very few of which a clinic will have any control over. You can help to reduce the chances of an IVF miscarriage happening to you if you take the lifestyle advice from my guides ‘Boost Female Fertility Naturally’ and ‘A Man’s Guide to Supercharging His Sperm’.
Multiple Pregnancies
If more than one embryo is transferred during IVF, it increases the risk of multiple pregnancies. Multiple pregnancies are where you become pregnant with more than one baby at the same time, i.e. twins, triplets, quadruplets or more. Though no fertility clinic should transfer more than three embryos at a time. Multiple pregnancies increase the risk of preterm births, placental problems, preeclampsia, and diabetes, as well as other less common problems. The number of embryos that will be transferred should be discussed before treatment starts and usually depends on your age and how many attempts at IVF you have had. As a rough rule of thumb, women under 37 years old should only receive one embryo. Women aged 37 to 40 should only receive two embryos if they have tried and failed previous courses of IVF. Older women may have two embryos transferred as a matter of course. The additional procedure of Assisted Hatching also carries a slightly increased risk of identical twins.
Premature Delivery and Low Birth Weight
IVF slightly increases the risk that the baby will be born early (before 37 weeks) or with a low birth weight. These can carry several risks for the baby including infection, breathing difficulties, nervous system problems, digestive problems and Sudden Infant Death Syndrome (SIDS).
Birth Defects
There is little evidence that IVF can cause birth defects in babies. However, women who have IVF tend to be older than those who don’t. Older women do have a slight increased risk of their children having birth defects whether they are having IVF or not. Though research has shown that older women who use younger eggs for IVF (either their own that have been frozen from earlier in their life or from a younger donor), have a reduced risk of birth defects. It is also worth noting that men over the age of 40 also have a slightly increased risk of having children with birth defects.
Other Risks and Side-Effects of IVF
The risks I have described above are the most common ones associated with IVF. There are others like mood swings, headaches, loss of appetite, or sleep problems. This is especially true if you or your partner are suffering from certain conditions. Furthermore, each medication that you take for these conditions will have its own list of possible side effects. Make sure your fertility clinic goes through all of them with you so you know what you might getting into. And if you experience anything out of the ordinary, inform your fertility clinic or family doctor immediately.
IVF Tips for Success
Some couples will go for IVF without having fully given lifestyle improvements for a natural birth a whole-hearted go. Instead, they see IVF as a shortcut so they don’t have to go on the diet or cut down on the party life. Well, I’ve got news for you. IVF is more likely to work if both you and your partner do the lifestyle changes recommended in my guides ‘Boost Female Fertility Naturally’ and ‘A Man’s Guide to Supercharging His Sperm’.
This is simply because an improved lifestyle increases the chances of becoming pregnant and maintaining a pregnancy. Be it through natural means, IVF, or any other fertility treatment.
Because IVF can be expensive and stressful, you want it to work in as few goes as possible. So why not properly try the lifestyle changes in these pages to get pregnant naturally beforehand? You are going to have to do them for IVF anyway if you want to have the best chance of that working.
Selecting a Fertility Clinic
The first and most important step towards IVF is selecting the fertility clinic that is right for you. Choosing the right clinic can help take away some of the stress and anxiety of the process. It can also save you from paying over the odds. Most importantly, choosing the right clinic can increase your chances of getting pregnant. For a detailed step-by-step guide on selecting the right fertility clinic for you, check out my guide here: How to Select the Best Fertility Clinic for You
Links to Popular Related Pages





